UDK: 615.387:611.018.52
Nancheva J.1, Bogoevska A.2, Andonovska N.1
1University Clinic for Traumatology, Orthopedic Disease, Anesthesiology, Reanimation and Intensive Care Medicine and Emergency Department, Faculty of Medicine, Ss. Cyril and Methodius University, Skopje, R.N Macedonia
2PHI City General Hospital “8th September” – Skopje
Abstract
Importance: Platelet transfusions are lifesaving in specific clinical contexts, particularly for patients with thrombocytopenia (low platelet counts) or platelet dysfunction. However, the procedure is not without risks. Platelets are biologically active and prone to cause immune and non-immune adverse events more frequently than red blood cell transfusions.
Objective: To provide recommendations in adult and pediatric populations in whom platelet transfusions are commonly performed.
Evidence Review: The new platelet transfusions guidelines established by the Association for the Advancement of Blood and Biotherapies (AABB) and the International Collaboration for Transfusion Medicine Guidelines (ICTMG), including Grading of Recommendations Assessment Development and Evaluation (GRADE) methodology were based on data of 21 randomized controlled trials and 13 observational studies all of which examined transfusion strategies using restrictive or liberal amounts of platelets. The authors noted that overall evidence demonstrated that restrictive transfusion strategies were not associated with increased risk of mortality, or increased bleeding, in most patient populations.
Keywords: anesthesia; platelets; surgery; platelets transfusion.
Introduction
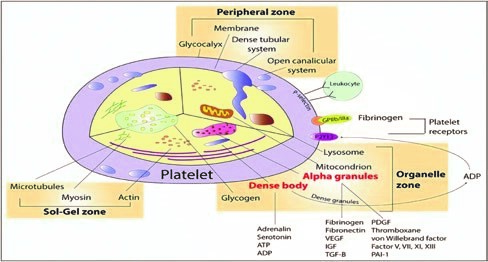
Circulating thrombocytes or platelets are anuclear discoid cells derived from bone marrow from megakaryocytes during fragmentation. Thrombopoietin is the main growth factor controlling megakaryocyte production. The circulating life span of native platelets is approximately 10 days, and that of transfused platelets is approximately 3 days in a stable recipient. Platelets have receptors on their surface and granules inside, allowing them to participate in adhesion, aggregation, and clot formation on the surface of injured endothelium, forming a haemostatic plug.
The number of circulating platelets for in adults ranges between 150 × 109/L and 450 × 109/L. Decreased number of platelets (thrombocytopenia) refers to any situation where the patient’s platelet concentration is below 150 × 109/L, in an adult. Both thrombocytopenia and platelet dysfunction without thrombocytopenia can cause bleeding. Actively bleeding patients might require support from platelet transfusions. Platelets are also used for prophylactic transfusions
Macedonian Journal of Anaesthesia
to prevent bleeding in patients with platelet production undergoing chemotherapy, and/or haematopoietic stem cell transplantation (HSCT). In addition, platelets are transfused to patients who have an increase in platelet destruction/consumption.
Causes of thrombocytopenia
Patients undergoing chemotherapy, HSCT, and those with chronic infections can have decreased platelet production. Another common cause of thrombocytopenia is an increase in platelet destruction/consumption that can have an immune (20%) or non-immune aetiology (80%) . Immune-mediated thrombocytopenia (ITP) is caused by different types of antibodies (autoimmune or alloimmune) that are produced to different platelet antigens and lead to elimination of the platelets in the spleen. Non-immune mechanisms cause platelet consumption and/or sequestration due to bleeding, enlarged spleen (sequestration) or vascular thrombi formation. It is not uncommon to have a combination of both immune and non-immune causes.
Decreased platelet production
- Chemotherapy;
- Preparation for and recovery from HSCT (including conditioning treatment with chemotherapy and sometimes radiation therapy);
- Radiation therapy;
- Aplastic anaemia and other bone marrow failure syndromes;
- Bone marrow suppression or infiltration due to chronic infections (e.g., tuberculosis, malaria, visceral leishmaniasis [kala-azar]).
Increased platelet destruction/consumption
Immune
- ITP;
- Drug-induced ITP (e.g., heparin-induced thrombocytopenia);
Supplement Vol. 10 No 1, February 2026 57
- Neonatal alloimmune thrombocytopenia;
- Post-transfusion purpura.
Non-immune
- Febrile state;
- Thrombotic microangiopathies (e.g., thrombotic thrombocytopenic purpura, haemolytic uraemic syndrome);
- DIC;
- Active bleeding;
- Splenic sequestration;
- Cavernous hemangioma.
Doses of prophylactic platelates
An adequate dose for prophylactic platelet transfusions is 1 apheresis unit (without Le, and from one donor) or a dose of 4–5 pooled whole-blood-derived platelet units (from several donors) for an average-size adult (70 kg). Whena smaller-than-expected increase in the platelet count increment occurs after transfusion of an adequate platelet dose, platelet refractoriness should be considered. One unit of random donor platelets derived from a unit of whole blood can increase the platelet count in an average-sized adult by 5,000–10,000/μL. Therefore, a dose of one random donor platelet per 10 kg of body weight is generally recommended. Pooled platelets prepared by pooling 4–6 units of whole blood-derived platelets can give a post-transfusion increment of 20,000 to 40,000/μL in an average-sized adult. The same increment would be expected from a dose of apheresis platelets.
New recommendations on platelet transfusions
The Association for the Advancement of Blood and Biotherapies (AABB) in partnership with the International Collaboration for Transfusion Medicine Guidelines (ICTMG), developed New Platelet Transfusions Guidelines published on 29 May, 2025 in JAMA.
The new guidelines offer recommendations for transfusion based on specific patient criteria, and these vary depending on individual patients’ needs. In general, the guidelines support the implementation of restrictive platelet transfusion strategies.
The authors of the new guidelines, led by Ryan Metcalf, MD, from the Department of Pathology at the University of Utah, noted that restrictive strategies reduce the risk of adverse reactions, mitigate platelet shortages, and reduce costs. “It is good practice to consider overall clinical context and alternative therapies in the decision to perform platelet transfusion,” they wrote.
The guidelines were based on data from 21 randomized controlled trials and 13 observational studies, all of which examined transfusion strategies using either restrictive or liberal platelet transfusion strategies. The authors noted that overall evidence demonstrated that restrictive
Macedonian Journal of Anaesthesia
transfusion strategies were not associated with increased risk of mortality or increased bleeding in most patient populations.
Recommendations
The authors categorized their recommendations based on the degree of evidence. They developed the following recommendations, considered to be “strong recommendations with high/ moderate-certainty evidence”:
- To address hyperproliferative thrombocytopenia in nonbleeding patients receiving chemotherapy or undergoing allogeneic stem cell transplant, platelet transfusion is recommended when the platelet count is less than 10×103/µL.
- For consumptive thrombocytopenia in neonates without major bleeding, platelet transfusion is recommended when the platelet count is less than 25×103/µL.
- In patients undergoing lumbar puncture, platelet transfusion is recommended when the platelet count is less than 20×103/µL.
- In patients with consumptive thrombocytopenia due to dengue without major bleeding, platelet transfusion is not recommended.
The authors also developed guidelines for additional patient populations but noted that these are “conditional recommendations with low/very low-certainty evidence.”
These recommendations include:
- For hypoproliferative thrombocytopenia in nonbleeding adults undergoing autologous stem cell transplant or with aplastic anemia, prophylactic platelet transfusion is not recommended.
- In adults with consumptive thrombocytopenia without major bleeding, platelet transfusion is recommended when the platelet count is less than 10 x103/µL.
- In adults undergoing central venous catheter placement in compressible anatomic sites, platelet transfusion is recommended when the platelet count is less than 10 x103/µL.
- In adults undergoing interventional radiology, platelet transfusion is recommended when the platelet count is less than 20 x103/µL for low-risk procedures and less than 50 x103/µL for high-risk procedures.
- For adults undergoing major nonneuraxial surgery, platelet transfusion is recommended when platelet count is less than 50 x103/µL.
- For nonthrombocytopenic patients undergoing cardiovascular surgery in the absence of major hemorrhage, including those receiving cardiopulmonary bypass, platelet transfusion is not recommended.
- For nonoperative intracranial hemorrhage in adults with platelet count more than
100 x103/µL, including those receiving antiplatelet agents, platelet transfusion is not recommended.
Supplement Vol. 10 No 1, February 2026 59
Comments
Claudia Cohn, MD, PhD, AABB’s chief medical officer and one of the authors of the guidelines, said these new guidelines were an important advancement for optimal transfusion strategies. “These new evidence-based guidelines move the field forward for many different patient populations,” Cohn said. “Overall, the guidelines prioritize patient safety and help conserve the limited platelet inventory.” In a related commentary published in Transfusion (June 2025), the authors underscored two major findings that informed the development of the new guidelines. First, they found that there is no consistent evidence that liberal platelet transfusion strategies improve mortality or reduce bleeding; and second, while current data support restrictive practices, the review found that the quality of the evidence varies substantially across patient populations.
Reference:
- Metcalf RA et al. Platelet Transfusion: 2025 AABB and ICTMG International Clinical Practice Guidelines. JAMA. Published online May 29, 2025.
- Anesthesia Updates on the NYSORA Anesthesia Manual App.